

We’ve all seen the CVS commercials — I told Felicia, my beautiful wife of 37 years, “Watch, you’re going to see many more of these commercials” — and according to Tennessee House Speaker Cameron Sexton, that $3 million advertising blitz is a textbook fear campaign designed to cloud a simple truth exposed by a sweeping state audit: CVS Caremark has been systematically overpaying its own pharmacies, burying spread pricing, and shortchanging rural communities — a problem I first learned about from my late stepfather, Dr. William “Bill” Chance, who opened the first Walgreens in Tennessee in Green Hills as a manager around 1958 and later served as a Tennessee State Investigator for the Board of Pharmacy, and who warned of these abuses long before they became headlines — while entrepreneur Mark Cuban’s Cost Plus Drugs proves transparent, fair drug pricing is not only possible, but already happening.
President Trump has signed H.R. 7148, the Consolidated Appropriations Act, 2026, into law. This major legislative package includes House Budget Chairman Jodey Arrington’s Better Deals and Lower Prices Act, delivering long-overdue transparency and accountability to pharmacy benefit managers (PBMs) to help lower prescription drug costs for American businesses and working families.
Key Provisions
The law mandates PBMs to pass through 100% of rebates, fees, and other remuneration to group health plans, effective for contracts 30 months after enactment. It also requires detailed semi-annual reports on drug pricing, rebates, and affiliate pharmacy incentives, plus annual reporting and audits for Medicare Part D PBMs.
Legislative Timeline
The House passed H.R. 7148 on January 22, 2026, on a bipartisan basis (341-88 vote). President Trump signed it into law by early February 2026.
Arrington’s Statement
“While America leads the world in medical innovation, our prescription drug delivery system has fundamental flaws that drive up costs for patients and taxpayers alike. This week, President Trump took a BIG step toward fixing that by signing my Better Deals and Lower Prices Act into law as part of H.R. 7148.” President Trump’s Great Healthcare Plan targets PBMs as “large brokerage middlemen” who have “deceptively” raised premiums, urging Congress to eliminate kickbacks fueling their profits and influence over drug pricing.
By increasing transparency around prescription drug pricing and PBM practices, this new law empowers consumers with the information they need to make  informed decisions, injects much-needed competition into the health care
informed decisions, injects much-needed competition into the health care
market, and helps ensure taxpayer dollars are spent in the most cost‑effective way. The result is intended to be lower prices, lower premiums, and a system that works better for both patients and taxpayers.
I’m proud to have led on these commonsense reforms that will drive down health care costs and deliver better deals for hardworking American families.” – Chairman Jodey Arrington.
Why Do Americans Pay So Much for Medicine?
The United States pays more for prescription drugs than any other country — and by a lot. American drug prices are nearly three times higher than in most other wealthy nations. The reason is simple: other countries set limits on what drug companies can charge. America doesn’t. Instead, we rely on a maze of private insurance companies and behind-the-scenes middlemen who, believe it or not, often make more money when drug prices go up. On top of that, pharmaceutical companies spend billions advertising directly to patients on TV — something most other countries don’t even allow — which drives up demand for expensive brand-name drugs and keeps prices sky high.
The people paying the price are everyday Americans. The same cancer drug that costs $81,000 in Germany runs over $200,000 here. Insulin — a medicine that’s been around for over a hundred years — can cost an uninsured American $3,000 a month just to stay alive. Nearly one in four Americans has trouble affording their medication, and millions more cut their pills in half or skip doses just to make ends meet. Every president promises to fix it. Not much changes. As long as drug companies are free to charge whatever they want, Americans will keep paying more than anyone else on earth for the privilege of getting well.
Alarming Tennessee Audit Findings
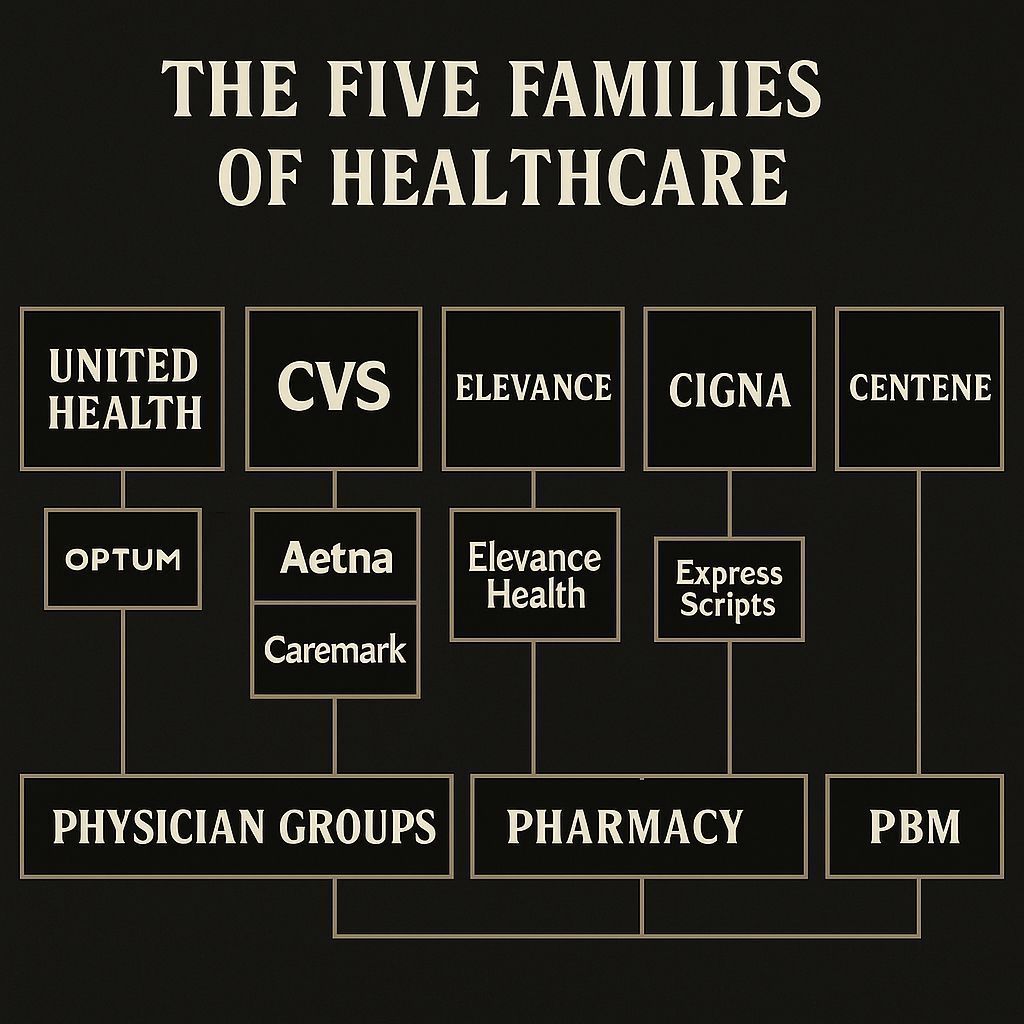
Tennessee’s recent audit of CVS’s pharmacy benefit manager (PBM), Caremark, alleges widespread violations of state PBM laws and has become a flashpoint in the broader debate over drug pricing, pharmacy access, and corporate consolidation in health care.

Background: Why Tennessee Audited CVS Caremark
In 2022, the General Assembly passed major PBM reform (Public Chapters 998 and 1070), giving the Tennessee Department of Commerce and Insurance (TDCI)clear authority to license, regulate, and audit PBMs operating in the state. Under that authority, TDCI conducted a comprehensive audit of Caremark’s 2024 operations in Tennessee, focusing on reimbursement practices, spread pricing, transparency, appeals, and network rules. Caremark is the PBM arm of CVS Health, one of the “Big Three” PBMs that collectively control most of the prescription claims market.
Key Findings from the PBM Audit
The TDCI audit identified 11 formal findings and five additional observations documenting systemic noncompliance with Tennessee PBM requirements.
Major findings included:
• Discriminatory reimbursements: CVS‑affiliated pharmacies were reimbursed at significantly higher rates than unaffiliated community pharmacies for the same drugs, with differentials as high as 16,510% for Cinacalcet 60 mg and 9,927% for Tadalafil 20 mg in sampled claims.
• Banned spread pricing: Despite Tennessee’s ban on spread pricing since 2021, TDCI found Caremark continued using spread pricing in contracts entered into and renewed after the law took effect, charging certain plans more than it paid dispensing pharmacies.
• Underpayment of professional dispensing fees: Caremark failed to pay required enhanced dispensing fees to low‑volume and rural pharmacies in a material share of tested claims, either paying no fee or the wrong amount.
• Appeals and transparency violations: The audit cited failures in the statutory appeals process, including improper denials and untimely payments, plus transparency gaps that hindered pharmacies and plan sponsors from understanding pricing and reimbursement methodologies.[yahoo +2]
These findings were formally adopted in a February 2026 order issued by TDCI, following earlier consent orders with CVS Caremark entered in September 2025 and January 2026.
Impact on Pharmacies, Patients, and Taxpayers
Tennessee pharmacists have long argued that PBM business practices are squeezing independent and rural pharmacies out of the market and limiting patient choice. The audit appears to validate those concerns by documenting that CVS‑owned pharmacies were paid dramatically more than competitors for many of the same prescriptions, while other pharmacies often did not receive the dispensing fees state law requires.
For patients and plan sponsors (including employers and public programs), spread pricing means higher costs without added clinical value: the PBM charges the health plan more than it pays the pharmacy, keeping the difference as profit even when state law is supposed to require a pass‑through or no‑spread model. A separate state audit of the CVS Caremark PBM contract for the State of Tennessee’s own employee health plan previously documented multimillion‑dollar reconciliation and rebate adjustments, underscoring the stakes of PBM oversight for taxpayers as well.
Legislative and Political Fallout
The audit has energized a new wave of PBM‑reform legislation at the Tennessee General Assembly. Lawmakers are considering bills that would:
• Tighten enforcement of Tennessee’s prohibition on discriminatory reimbursement and spread pricing.
• Strengthen transparency requirements so plan sponsors can see exactly what PBMs pay pharmacies versus what they bill the plan.
• In at least one measure (SB 2040/HB companion), bar PBMs from owning pharmacies, forcing vertically integrated companies like CVS to choose between operating a PBM or a retail chain in Tennessee.
In response, CVS has warned that such legislation could lead to closure of its 100‑plus Tennessee pharmacy locations, framing the reforms as a threat to access and affordability. Supporters of the bills argue that access is already under threat when independent and rural pharmacies cannot survive under current PBM payment structures and that true competition requires fair reimbursement and transparent pricing.
Why This Audit Matters Beyond Tennessee
The Tennessee Pharmacists Association called the TDCI audit a “blueprint” for PBM reform nationally, pointing to the combination of strong statutory authority, detailed auditing, and public reporting as a model for other states. National pharmacy and legal organizations have highlighted the audit as evidence of how vertically integrated PBMs can leverage market power in ways that disadvantage competitors and distort drug pricing.
At a time when prescription drug affordability is a top concern for voters and policymakers, the CVS Caremark PBM audit in Tennessee illustrates how the “middleman” in the drug supply chain can impact everything from what a local pharmacy is paid to what a state Medicaid program or employer ultimately spends on medications.
Mark Cuban Sparks Disruptions in the Pharmaceutical Marketplace
Mark Cuban’s Cost Plus Drugs slashes prices by up to 90% with transparent, no-middleman pricing.
Leave feedback about this